Tennis Elbow: Causes, Symptoms, and How Physiotherapy Treats It

Tennis elbow is an overuse condition of the tendons on the outside of the elbow, and most cases settle with the right plan rather than a procedure. This guide explains what tennis elbow is, why it happens, how to recognize it, and how a structured tennis elbow treatment built around physiotherapy can help you load the tendon back to full capacity.
Key takeaways
- Tennis elbow (lateral epicondylitis) is an overuse injury of the wrist extensor tendon at the lateral epicondyle, not a tennis-only problem.
- Typical signs are pain and tenderness on the outside of the elbow, worse with gripping, lifting, or wrist extension.
- Most cases improve with conservative care, though recovery can be gradual and may take several months.
- Education, load modification, and progressive strengthening of the wrist extensors are the cornerstones of physiotherapy.
- Injections, shockwave, PRP, and surgery are reserved for selected stubborn cases, not first-line care.
What is tennis elbow, and why does it happen?
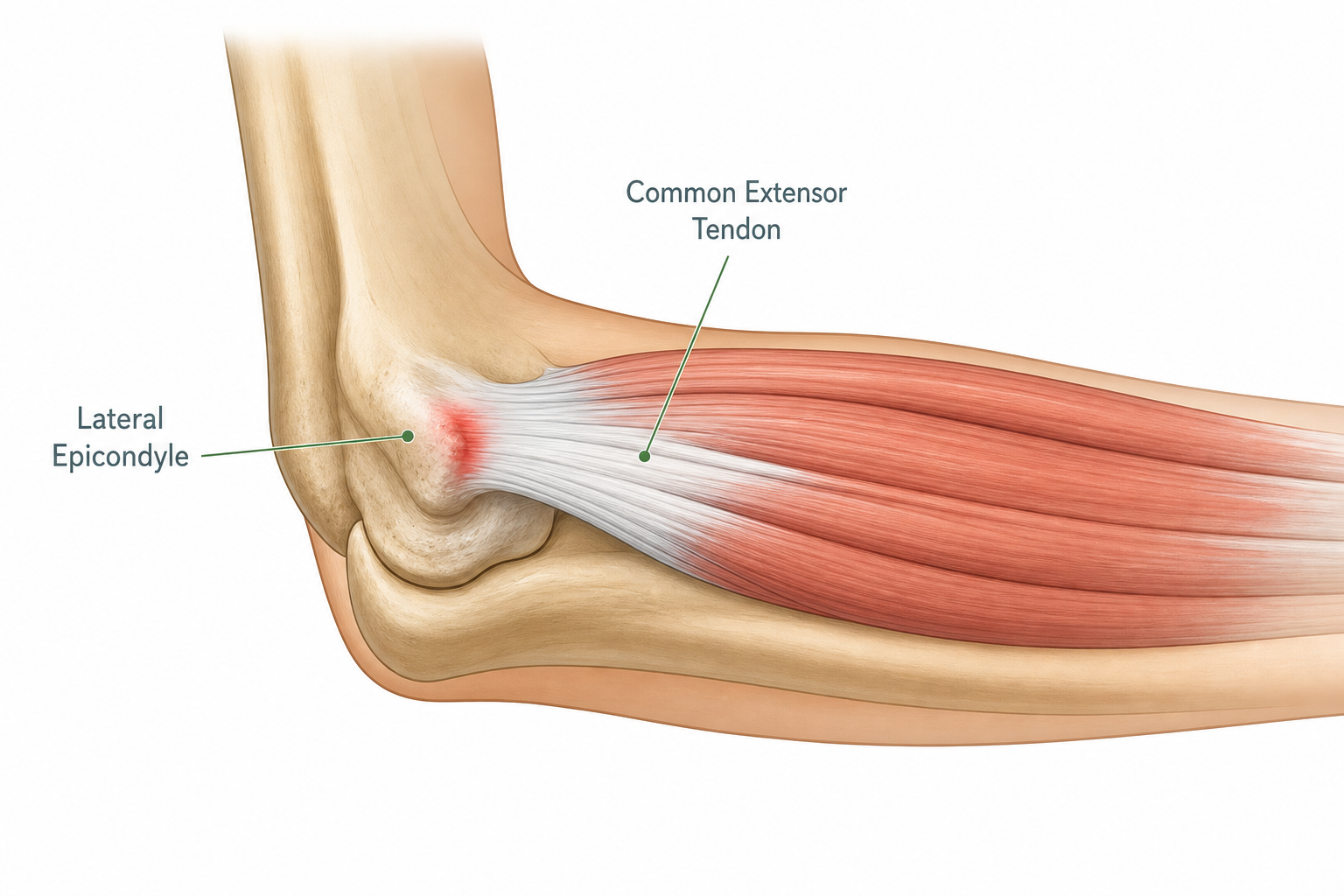
If the outside of your elbow has been niggling every time you grip a kettle, twist a screwdriver, or shake a hand, you are not alone. We understand how this kind of pain can quietly chip away at your day, and the good news is that it is usually very treatable. Tennis elbow, known clinically as lateral epicondylitis or lateral epicondylalgia, is an overuse condition affecting the common wrist extensor tendon where it attaches to the lateral epicondyle on the outside of your elbow.
Despite the name, most people who develop tennis elbow have never picked up a racket. It is the repetition, not the sport, that matters. The condition is typically triggered by repeated gripping, wrist extension, forearm twisting, or other repetitive use of the forearm, whether that is hours of typing and mouse work, swinging tools on a building site, lifting babies and toddlers, or playing a sport with poor technique. Over time, the tendon at the lateral epicondyle becomes irritated and structurally unhappy, and the body struggles to keep up with the demand placed on it.
Although the older term epicondylitis implies pure inflammation, current understanding sees the condition as more of a failed healing response in the tendon. That nuance matters, because it tells us why simply resting or taking anti-inflammatories rarely fixes the problem on its own. The tendon needs a reason to remodel, and that reason is graded, controlled load.
Where the pain comes from
The pain of tennis elbow sits squarely on or just below the bony bump on the outside of your elbow. From there it can radiate down into the forearm, especially when you grip, lift, or rotate. Patients often describe it as a deep, dragging ache that flares with specific tasks: pouring a heavy pan, opening a jar, lifting a laptop, or shaking hands.
Three features are typical:
- Localized tenderness when you press on the outside of the elbow, right over the lateral epicondyle.
- Pain on resisted wrist extension, the classic tennis elbow test a clinician uses, where lifting the back of the hand against resistance reproduces the familiar pain.
- Pain with gripping, especially with the palm facing down, which loads the wrist extensors hardest.
Many people also notice the symptoms creep into their work and home routines, with computer use, repetitive machinery, or carrying shopping becoming surprisingly provocative. If that sounds familiar, a focused course of tennis elbow physiotherapy can help you make sense of the pattern and start changing it.
How is tennis elbow diagnosed?
Tennis elbow is largely a clinical diagnosis. During an assessment, one of our doctors will take a careful history of your activities, examine the elbow, and run a few simple loading tests to confirm the source of the pain and rule out other causes such as cervical referral, nerve entrapment, or joint pathology. Imaging is not usually needed for a straightforward presentation, although it may be considered if symptoms behave unusually or have not responded to good conservative care.
Other things it could be
Not every ache on the outside of the elbow is tennis elbow. Radial nerve irritation, referred pain from the neck, and elbow joint problems can mimic it, which is one reason a proper orthopedic physiotherapy assessment is so useful before settling on a plan.
The best treatment for tennis elbow: what the evidence says
People often ask us, what is the best treatment for tennis elbow, and what is the treatment for tennis elbow pain in the long run? The honest answer from current guidance is that the best treatment is rarely a single thing. It is a multimodal, individualized rehabilitation plan built around education, sensible load management, and progressive strengthening. Reviews of recent evidence consistently put eccentric or combined strengthening, ergonomic advice, and patient education at the heart of conservative care.
Most cases of tennis elbow are self-limiting and improve without injections or surgery, with many resolving over a period of about six to twelve months. Recovery can feel slow, but it is usually steady when the plan is right. Our approach to tennis elbow treatment in Dubai reflects that evidence base, blending hands-on care with a clear strengthening program you carry through the week.
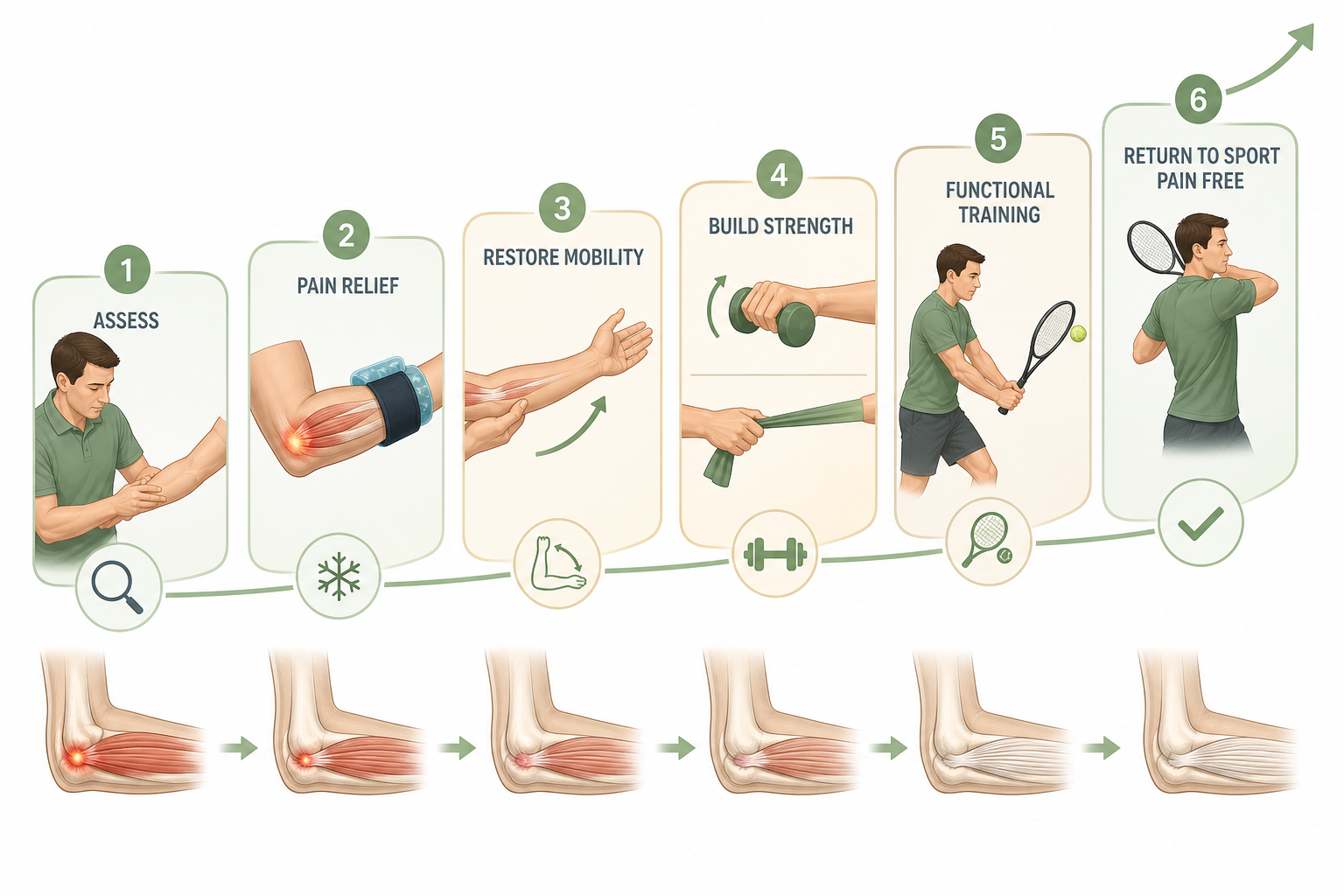
A typical physiotherapy treatment of tennis elbow includes several layers working together:
- Education and load modification. Understanding which movements provoke the tendon, and adjusting how, not whether, you do them.
- Progressive strengthening of the wrist extensors, often using eccentric or heavy-slow protocols, supported by forearm, grip, and shoulder work.
- Manual therapy as an adjunct, including soft-tissue work and joint mobilization where it helps reduce pain and improve movement.
- Symptom-modulating tools such as taping, a counterforce brace, ice or heat, and short-term pain-relief strategies to help you tolerate loading.
- Ergonomic and technique review for the desk, the workshop, or the sport, so the tendon is not being asked to do the same provoking job all day.
Pro tip
If gripping is your main aggravator, try turning your palm to face up when you can. Carrying a bag or lifting a kettle with the forearm supinated loads the wrist extensors much less than the classic palm-down grip.
Exercises that help
Exercise is the part of the plan that does the heavy lifting over time. Passive treatments can feel good in the moment, but stronger, better-conditioned tendons are what reliably keep tennis elbow from coming back. Tennis elbow exercises are usually introduced gently and progressed week by week as pain allows.

A simple, well-tested starting point looks like this:
- Isometric wrist extensor holds. Resting your forearm on a table, palm down, hold a light weight or resistance band against gentle wrist extension for around 30 to 45 seconds, several repeats. Useful early on when movement is irritable.
- Eccentric wrist extensions. Lift the wrist up with help from the other hand, then slowly lower the weight back down over three to five seconds. The slow lowering is the active ingredient.
- Heavy-slow strengthening. As pain settles, progress to controlled wrist extensions with a heavier weight, two to three sets, several days a week.
- Grip work. Squeezing a soft ball or a stress putty for short holds builds grip tolerance for everyday tasks.
- Forearm and shoulder support. Strengthening the rotator cuff, scapular stabilizers, and forearm rotators reduces the load funnelling through the elbow.
The aim is not to chase pain away on each rep. A mild, tolerable discomfort during exercise that settles within 24 hours is usually acceptable, and progress comes from consistency rather than intensity. Your physiotherapist will calibrate this carefully so the tendon is loaded enough to adapt, but not flared.
Everyday habits to change
Treatment for tennis elbow at home is largely about taking pressure off the tendon while you let strengthening do its work. Small habit changes, repeated all day, often matter more than any single exercise.

Useful adjustments include:
- Lift with the palm up whenever possible. Avoid lifting heavy objects with the forearm fully pronated and the palm facing down when the elbow is painful.
- Spread the load. Use both hands for jugs, pans, and shopping bags. Choose larger, softer grips on tools and pens.
- Break up repetition. If your work involves typing, mousing, or tool use, build in short, frequent micro-breaks rather than one long pause.
- Set up your workstation so the wrist sits in a neutral position. A supportive mouse, a softer keyboard, and a properly heighted desk all matter.
- Warm up before sport or heavy DIY, and progress training load gradually rather than in big jumps.
- Consider a counterforce brace for provocative tasks, as a short-term aid that helps you stay active while the tendon settles.
Clinical guidance specifically discourages prolonged rest or full immobilization. Staying gently active, within a tolerable threshold, is more helpful than wrapping the arm up and waiting. Where you do need calm, controlled hands-on input, our manual therapy sessions sit alongside your home program, not instead of it.
When physiotherapy is not enough: injections, shockwave, and surgery
Most people improve with the conservative plan above. For a smaller group, symptoms persist despite appropriate care, and additional options are considered. These are not first-line treatments, and the evidence varies, but they have a place in selected refractory cases.
Options sometimes discussed include a tennis elbow injection (corticosteroid or other agents), platelet-rich plasma (PRP) treatment for tennis elbow, shockwave therapy, dry needling, and, rarely, surgery. PCD does not perform surgery or injections; what we can offer is shockwave therapy as part of a carefully selected plan, along with coordinated rehabilitation if you do have an injection or operation elsewhere.
| Approach | What it is | Where it fits |
|---|---|---|
| Education and load modification | Understanding triggers, adjusting daily tasks | First-line, for every case |
| Progressive strengthening | Eccentric and heavy-slow wrist extensor work | Core of conservative care |
| Manual therapy | Soft-tissue work, joint mobilization | Helpful adjunct, not stand-alone |
| Taping or bracing | Counterforce brace, supportive taping | Short-term symptom relief |
| Shockwave therapy | Focused acoustic waves to the tendon | Considered when rehab plateaus |
| Injection or PRP | Corticosteroid, PRP, or other agents | Selected refractory cases, via a physician |
| Surgery | Tendon debridement or release | Rare, for persistent severe cases |
What about ayurvedic treatment for tennis elbow?
Many readers ask about tennis elbow ayurvedic treatment or tennis elbow treatment in ayurveda, sometimes after seeing content in Malayalam or other languages. Some people find traditional approaches such as oil massage or herbal preparations soothing alongside their rehabilitation, and that can be a reasonable personal choice. From a clinical standpoint, the strongest evidence for long-term improvement still points to progressive loading of the tendon, education, and activity modification. If you are using ayurvedic care, we are happy to work alongside it, and we will keep your physiotherapy plan grounded in what current research supports.
What to expect from a course of tennis elbow physiotherapy at PCD
Your first visit is a doctor-led assessment, usually with Dr. Mina Gamil or one of our senior physiotherapists. We listen carefully to how the pain behaves, examine the elbow, the wrist, the shoulder, and the neck, and identify the loads that are provoking the tendon. From there, we build a personalized plan that often combines hands-on treatment, a structured strengthening program, and clear ergonomic advice. If shockwave is appropriate, we discuss whether and when to introduce it.
Sessions are one-to-one, in the clinic, with the same clinician guiding your progression. Between visits, your home program does the day-to-day work. Recovery from tennis elbow is rarely linear; some weeks feel like clear progress, others feel flat, and that is normal. With consistent loading and sensible activity choices, most people see meaningful improvement over weeks to months. Patients managing more general elbow and arm symptoms often benefit from the same framework we use for broader orthopedic physiotherapy.
The goal is not just a quiet elbow today, but a forearm that copes with the gripping, lifting, and twisting your life actually asks of it.
When to see a physiotherapist
Book an assessment if the outside of your elbow has hurt for more than two to three weeks despite easing off, if pain is waking you at night, if gripping everyday objects has become difficult, if you notice numbness, tingling, or weakness in the hand, or if symptoms have not improved after a fair trial of self-care.
If your elbow has been holding you back, our team would be glad to help you build a plan that fits your work, your sport, and your goals. Message us on WhatsApp, call +971 50 301 3005, or book your free 30-minute consultation.
Related care at Physio Cure Dubai
Doctor-led services for what you have just read about.
Frequently Asked Questions
Need Help With Your Recovery?
Book a free consultation with our expert physiotherapists.
Related Articles

Sports Physiotherapy in Dubai: From Injury to Return to Play
Learn how sports physiotherapy dubai supports injury rehab, strength rebuilding, and return-to-play testing with doctor-led care in Dubai Silicon Oasis.
12 min read

Cupping for Muscle Recovery: Unlocking Peak Performance
Learn how dry cupping therapy speeds muscle recovery, flushes toxins, and boosts mobility for athletes. Explore timing, benefits, and expert-led treatment i
15 min read

Dry Needling for Athletes: Rapid Recovery & Peak Power
Doctor-led dry needling targets trigger points to relieve pain, accelerate recovery, restore mobility, and boost athletic performance for serious competitors.
15 min read